
Table of Contents
About
Latest Evidence-Based Guidelines
2.1 Advances in Detection and Imaging
2.2 Personalized Risk Stratification and Genetic Testing
2.3 Advanced Therapies and Clinical Trial Opportunities
2.4 Disparities and Population-Specific Risks
Resources and Emerging Diagnostic Tools
Future Directions in Personalized Care
The Top 10 Questions
References
Terminologies
Glossary
About
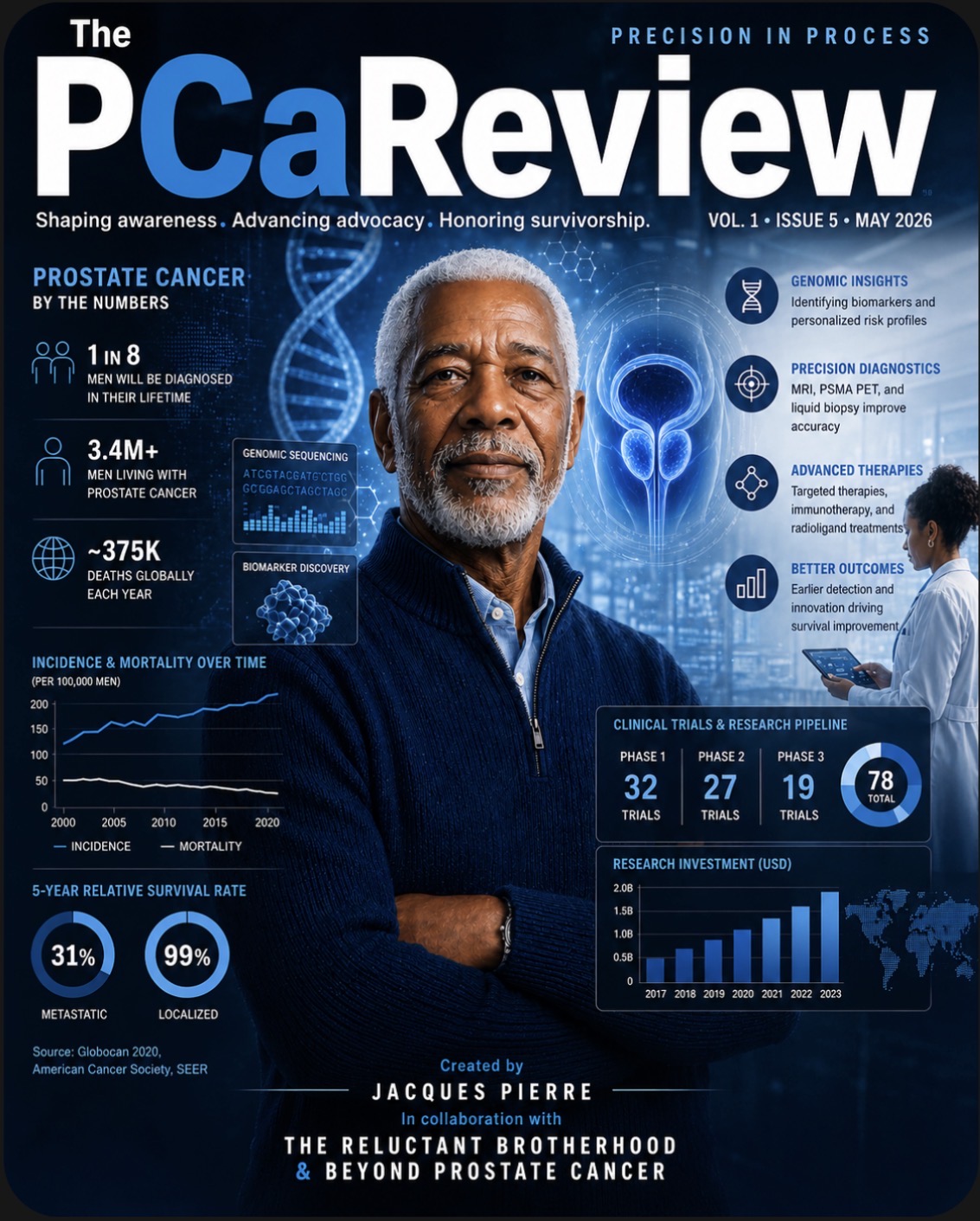
The PCaReview: Precision in Progress delivers monthly, curated, research-driven insights into the evolving field of prostate cancer care. This publication provides an overview of current advances, clinical guidelines, and personalized strategies for the diagnosis, treatment, and management of prostate cancer.
© 2026 All Rights Reserved
All content in this publication is protected under copyright law. No part of this magazine may be reproduced, distributed, or transmitted in any form without prior written permission from the publisher, except for brief quotations used in reviews or commentary.
Published by: Kristanara Grace
Editor-in-Chief: Jacques Pierre
Issue: Volume 1, Issue 5, May 2026
Contributor Notice
Unless otherwise stated, all articles, photographs, and illustrations are the property of their respective creators and are used in this publication under license or agreement.
Trademarks
All brand names and logos are the property of their respective owners.
Latest Evidence-Based Guidelines
2.1 Advances in Detection and Imaging
Prostate cancer screening and diagnosis are becoming more accurate and less invasive than in the past. Traditionally, doctors relied heavily on a single PSA blood test and random biopsies, which sometimes led to unnecessary procedures or missed more aggressive cancers.
Today, newer tools allow for a more personalized approach. Doctors can look at PSA trends over time (called PSA velocity) rather than a single number. Imaging tests like MRI can help pinpoint suspicious areas in the prostate, so biopsies can be more targeted. PSMA PET scans are advanced imaging tools that can detect prostate cancer more precisely, especially in certain higher-risk cases. In addition, some urine-based tests can help assess cancer risk without needing an immediate biopsy.
Together, these advances help doctors find clinically significant cancers earlier while reducing the chance of overtesting or overtreatment.
What this means for you:
You may be able to avoid unnecessary biopsies and get a clearer, more individualized understanding of your risk. Testing can be better tailored to your specific situation rather than using a one-size-fits-all approach.
What to ask your doctor:
Ask how your PSA has changed over time, whether an MRI could help guide decision-making before a biopsy, if you might benefit from a PSMA PET scan, and whether non-invasive options like urine tests are appropriate for you.
Sample Questions
- How should I interpret my PSA level for my age and risk?
- Would an MRI before a biopsy make sense for me?
- Am I a candidate for a PSMA PET scan or is that only for certain cases?
- Are there urine or other non-invasive tests I should consider?
- Based on my results, how likely is it that I have aggressive cancer?
- Do I need a biopsy now, or can we monitor safely?
- How can we minimize unnecessary biopsies or treatments?
2.2 Personalized Risk Stratification and Genetic Testing
Prostate cancer is no longer treated as a one-size-fits-all disease. Doctors now classify it into risk categories—low, intermediate, or high—based on a combination of clinical findings (such as PSA level, biopsy results, and imaging) and, in some cases, genetic information.
For men with low-risk cancer, active surveillance (closely monitoring the cancer without immediate treatment) is often a safe option. Intermediate-risk cases may require more selective treatment, while high-risk cancers typically call for a more aggressive approach.
Genetic testing is becoming an important part of this process. Some men carry inherited or tumor-related gene changes—such as BRCA1, BRCA2, or other homologous recombination repair (HRR) mutations—that can influence how the cancer behaves and which treatments may work best. For example, certain targeted therapies, including PARP inhibitors (often used alongside hormone therapy), may be more effective in men with these mutations.
Genetic counseling can also help you understand whether your results have implications for family members, who may share similar risks.
What this means for you:
Your treatment plan can be tailored to your specific level of risk, helping you avoid overtreatment if your cancer is low-risk—or ensuring you get more effective therapy if your cancer is more aggressive.
What to ask your doctor:
Ask which risk category you fall into, whether genetic testing is appropriate for you, and if active surveillance is a safe option in your case. Also ask if your results could open the door to targeted treatments.
Sample Questions
- What risk category am I in, and what does that mean for me?
- Is my cancer considered aggressive?
- Should I be tested for BRCA1, BRCA2, or HRR mutations?
- Would genetic testing results change my treatment options?
- Do I need treatment now, or is active surveillance safe?
- Am I a candidate for targeted therapies like PARP inhibitors?
- Would combination therapy be better in my case?
- What are my options if the cancer progresses?
Follow-up steps:
Confirm your risk category and ask whether a genetic testing panel or referral to a genetic counselor would be helpful.
2.3 Advanced Therapies and Clinical Trial Opportunities
For men with metastatic or treatment-resistant prostate cancer, new therapies are expanding treatment options and improving outcomes. These include targeted treatments such as PSMA radioligand therapy (for example, Lutetium-177 PSMA-617), PARP inhibitors for men with certain genetic mutations (like BRCA or other HRR mutations), and immunotherapy in select cases.
PSMA radioligand therapy works by delivering radiation directly to prostate cancer cells that express PSMA, a protein commonly found on these cells. PARP inhibitors target cancers with specific DNA repair weaknesses, while immunotherapy helps the immune system recognize and attack cancer—though it is effective only for certain patients.
Clinical trials are playing a key role in advancing these treatments. Researchers are studying how to use these therapies earlier in the disease, as well as in combination, to improve results. Participating in a clinical trial may provide access to cutting-edge treatments not yet widely available.
What this means for you:
If your cancer is advanced or no longer responding to standard treatments, you may have more options than ever before—including therapies tailored to your tumor’s specific features.
What to watch for:
Ask whether your cancer has PSMA expression (which may make you eligible for radioligand therapy), whether genetic testing shows mutations that could respond to targeted drugs, and whether there are signs that your current treatment is becoming less effective.
What to ask your doctor:
Ask if you are a candidate for newer treatments or combination therapies, and whether a clinical trial might be a good option for you.
Sample Questions
- Am I a candidate for PSMA-targeted treatments like Lutetium-177 therapy?
- Would immunotherapy or targeted therapy work for my type of cancer?
- Should we consider these newer treatments now or later?
- What signs indicate it's time to switch therapies?
- Am I eligible for any clinical trials right now?
- What trials are available locally or regionally?
- What are the risks and potential benefits of joining a trial?
- Do my genetic or tumor test results open specific treatment doors?
Follow-up steps:
Request a clinical trial eligibility screening and discuss testing (such as PSMA imaging or genetic profiling) that may help guide your next steps.
2.4 Disparities and Population-Specific Risks
Prostate cancer does not affect all men equally. While overall rates are rising, Black men are significantly more likely to be diagnosed with aggressive prostate cancer and are more than twice as likely to die from the disease compared to other groups.
Several factors contribute to this disparity. Genetics may play a role, but differences in access to early screening, timely diagnosis, and quality care are also major contributors. In many cases, delays in detection mean the cancer is found at a more advanced and harder-to-treat stage.
Because of these risks, a more proactive and personalized screening approach is especially important for men at higher risk—including Black men and those with a family history of prostate cancer. This may mean starting screening earlier, testing more frequently, and using additional tools beyond a standard PSA test when appropriate.
What this means for you:
Understanding your personal risk can help you and your doctor take earlier, more targeted steps to detect prostate cancer when it is most treatable.
What to ask your doctor:
Ask when you should begin screening, how often you should be tested based on your risk, and whether additional tools (like MRI or genetic testing) should be part of your plan.
Sample Questions
- Based on my background, am I at higher risk for aggressive prostate cancer?
- Should I be screened more frequently than average?
- When should I start or continue PSA screening?
- Are there additional tests I should consider because of my risk?
- How can we make sure we catch anything early?
- Would imaging or newer tests be appropriate for me?
- Am I receiving the same level of screening recommended for higher-risk patients?
- Should I see a specialist or seek a second opinion?
Follow-up steps:
Work with your doctor to create or review a proactive, risk-adjusted screening plan that reflects your personal and family history.
Resources and Emerging Diagnostic Tools
Major medical organizations regularly update their prostate cancer guidelines to help ensure patients receive the most effective and personalized care possible. Groups like the National Comprehensive Cancer Network (NCCN), American Society of Clinical Oncology (ASCO), and American Cancer Society (ACS) now emphasize a more individualized approach to screening, monitoring, and treatment.
Recent guideline updates highlight the growing role of advanced imaging tools such as MRI and PSMA PET scans, along with genetic testing to better understand a person’s risk and guide treatment decisions. These recommendations take into account factors like family history, inherited mutations (such as BRCA1 or BRCA2), overall risk level, and stage of disease when determining the best care plan.
Newer, less invasive monitoring tools are also becoming more widely used. Urine biomarkers and liquid biopsies can help detect signs of aggressive cancer or monitor progression using simple blood or urine samples, potentially reducing the need for repeated biopsies in some patients.
Because prostate cancer can vary significantly from person to person, following updated, evidence-based guidelines helps ensure that care is tailored to your specific needs and risk factors. It also gives patients access to newer technologies and treatment strategies that may improve outcomes and reduce unnecessary procedures.
What this means for you:
Staying informed about current prostate cancer guidelines can help you receive more personalized care, better monitoring options, and access to newer tools that support earlier detection and more targeted treatment.
What to ask your doctor:
Ask whether your care plan follows the latest NCCN or ASCO recommendations, whether advanced imaging or genetic testing may be appropriate for you, and if newer non-invasive monitoring tools could help guide your care. You can also ask how your personal risk factors influence your screening or treatment plan.
Sample Questions - Available Resources
- Are my screening and treatment decisions based on current NCCN or ASCO guidelines?
- Have there been any recent updates that apply to my case?
- How does my care plan compare to standard recommendations for someone like me?
- Are there alternative approaches supported by current guidelines?
- Are there trusted resources you recommend for me to learn more?
- Should I review information from Mayo Clinic or Johns Hopkins?
- Would a second opinion at a major cancer center be helpful?
- Are there specialists or centers you recommend?
Sample Questions - Diagnostic Tools
- Are there urine-based tests that could help decide if I need a biopsy?
- Would a liquid biopsy be useful in my case?
- How will we track my cancer over time without repeated invasive procedures?
- What tests are best for detecting early recurrence or progression?
- How reliable are these newer tests compared to standard approaches?
- Will the results actually change what we do next?
- Am I a good candidate for these newer monitoring tools?
- Are they recommended for someone at my stage or risk level?
Follow-up steps:
Review your treatment plan for guideline alignment and explore non-invasive monitoring options like urine tests or liquid biopsies.
Future Directions in Personalized Care
Prostate cancer treatment is becoming increasingly personalized, with doctors using advanced imaging, genetic information, and targeted therapies to tailor care to each individual patient. Rather than using the same approach for everyone, treatment decisions are now based on how aggressive the cancer appears, how likely it is to grow or spread, and how it may respond to specific therapies.
Advanced imaging tools such as PSMA PET scans and genomic profiling help doctors better understand the unique characteristics of a patient’s cancer. These tools can improve treatment planning, identify cancers that may need more aggressive care, and help avoid unnecessary treatment in lower-risk cases where active surveillance may be the safest option.
New non-invasive monitoring methods are also changing how prostate cancer is followed over time. Urine biomarker tests and liquid biopsies—which detect small amounts of cancer DNA in the blood—can help monitor treatment response, detect early signs of recurrence, and reduce the need for repeated biopsies in some patients.
Genetic testing is playing a larger role as well. Tumor-based tests such as Decipher can help predict how aggressive a cancer may be and estimate recurrence risk. Inherited genetic testing for mutations such as BRCA1, BRCA2, and other DNA repair genes may identify patients who could benefit from targeted therapies like PARP inhibitors, while also providing important information for family members who may share similar risks.
Clinical trials continue to drive many of these advances, giving patients access to emerging therapies and new treatment combinations designed to improve outcomes and quality of life. Because prostate cancer can change over time, treatment plans may also evolve, making shared decision-making between patients and doctors especially important.
What this means for you:
Personalized prostate cancer care may help avoid unnecessary treatments, improve monitoring, and provide access to therapies that are specifically matched to the biology of your cancer.
What to ask your doctor:
Ask whether advanced imaging, genomic profiling, urine biomarkers, or liquid biopsies may be appropriate for your care. You can also ask if inherited genetic testing or genetic counseling is recommended for you or your family, and whether any clinical trials may be a good fit for your situation.
Sample Questions - Genetics and Molecular Profiling
- Should I get a genomic test like Decipher on my tumor?
- What does my tumor biology say about how aggressive this cancer is?
- Do I need genetic testing for BRCA1, BRCA2, or HRR mutations?
- Would the results affect my treatment options?
- Am I eligible for targeted therapies based on my genetic profile?
- Would this information change whether I choose treatment or surveillance?
- Should my family members be tested if I have a mutation?
- Should I speak with a genetic counselor?
Sample Questions - Future Directions
- Is my treatment plan based on risk stratification and updated guidelines?
- How are imaging and genetic results influencing my care?
- Would advanced imaging like PSMA PET or MRI change my management?
- Should I have tumor or inherited genetic testing to refine treatment?
- How do we decide when to escalate or de-escalate treatment?
- What does "personalized care" mean in my specific case?
- Are there clinical trials that align with my condition?
- If my cancer changes, how quickly can we adjust my treatment plan?
Bottom line and follow-up steps:
This integrated approach—imaging + genomics + targeted therapies—delivers risk-adapted care that improves survival and quality of life. Review your ongoing plan, explore alternative testing, and consider trial options to stay at the forefront of care.
The Top 10 Questions
- What exact risk category am I in?
- Should I get genetic testing (BRCA/HRR/Decipher)?
- Am I eligible for clinical trials?
- Are we following current NCCN/ASCO guidelines?
- Would MRI or PSMA PET change my management?
- Is active surveillance safe for me?
- Are there urine tests to avoid biopsy?
- What does my PSMA expression mean for treatment?
- Should I get a second opinion at a major center?
- How often should I be screened based on my risk?
Conclusion
The more informed and prepared you are, the more confident and productive your conversations with your doctor can be. Prostate cancer care is evolving rapidly, and understanding your personal risk, screening options, and treatment choices can help you take an active role in your health.
Before your next appointment, consider writing down your questions, reviewing your family history, and bringing any recent test results or medication lists with you. No question is too small—clear communication helps ensure you receive care that is informed, personalized, and aligned with your goals.
References
American Cancer Society – 2025 Prostate Cancer Statistics Press Release https://pressroom.cancer.org/2025-Prostate-Cancer-Report
ACS Journal Article – Prostate Cancer Statistics, 2025 https://acsjournals.onlinelibrary.wiley.com/doi/full/10.3322/caac.70028
ASCO Living Guideline (2026.1) – Systemic Therapy in Metastatic Castration‑Resistant Prostate Cancer https://ascopubs.org/living-guideline/metastatic-castration-resistant-prostate
NCCN Clinical Practice Guidelines – Prostate Cancer, Version 3.2026 https://pubmed.ncbi.nlm.nih.gov/41213253/
Mayo Clinic – PSMA PET Scan for Prostate Cancer https://www.mayoclinic.org/tests-procedures/psma-pet-scan/about/pac-20582225
Urine‑based biomarker assay for prostate cancer (Johns Hopkins‑related) https://ascopost.com/issues/september-25-2025/new-nih-funded-study-identifies-urine-based-assay-for-prostate-cancer/
Prostate Cancer Foundation – 2026 Localized Prostate Cancer Patient Summit https://www.pcf.org/patient-support/patient-summits/2026-localized-prostate-cancer-patient-summit/